Primary Aldosteronism is a Disease of the Adrenal Glands
Hormones are chemical messengers that regulate key bodily functions such as metabolism, growth, blood pressure, electrolytes balance, reproduction, sleep, and even mood. Every cell in the body has receptors for specific hormones that, when activated, cause the cell to take certain actions.
Hormones are also used to coordinate action between glands through complex feedback loops to keep the body’s system in balance or to respond to changes in the environment.
Primary aldosteronism is an endocrine disease that can affect one or both adrenal glands, and is most often caused by a benign tumor or by excess growth of aldosterone-producing cell clusters in both adrenal glands, termed bilateral hyperplasia.
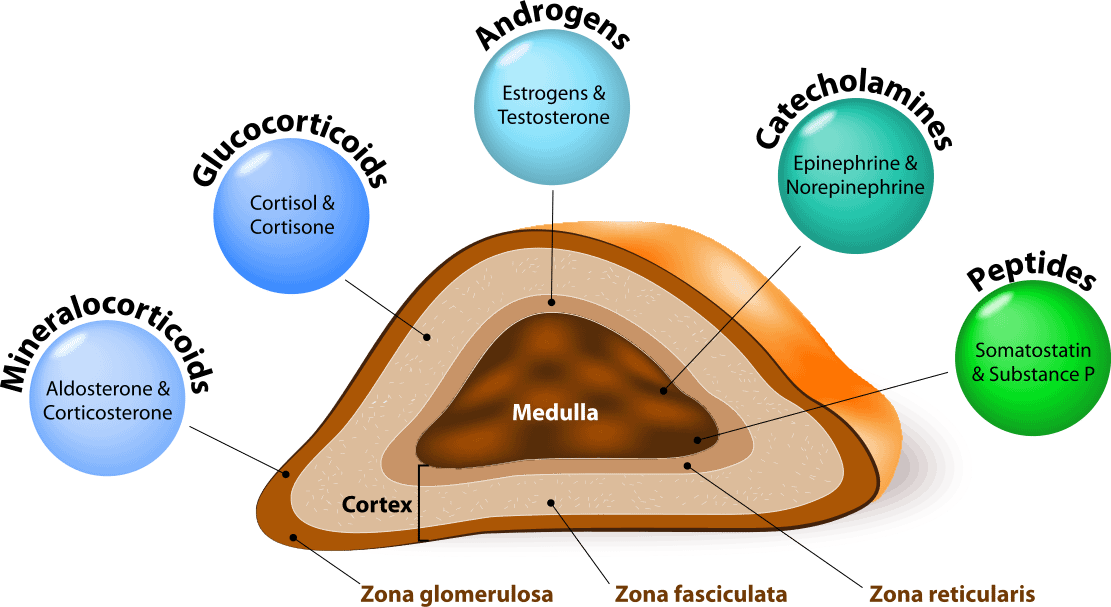
An essential part of the endocrine system, the adrenal glands are very small triangular-shaped organs which sit atop of the kidneys. The adult adrenal glands weigh some 4 to 5 grams each (less than 1/5th of an ounce). Aldosterone is produced by the outer most layer (glomerulosa) of the cortex of the adrenal glands. Besides aldosterone, adrenal glands also produce and excrete cortisol, adrenaline, epinephrine, and sex hormones into the blood stream.